Causes
One proposed cause of pilonidal cysts is ingrown hair, although hairs found in pilonidal sinus tracts may originate from the head. Excessive sitting is thought to predispose people to the condition, as sitting increases pressure on the coccygeal region. Trauma is not believed to cause a pilonidal cyst; however, such an event may result in inflammation of an existing cyst; there are cases where this can occur months after a localized injury to the area. Pilonidal cysts may be caused by a congenital pilonidal dimple. Excessive sweating can also contribute to the formation of a pilonidal cyst: moisture can fill a stretched hair follicle, which helps create a low-oxygen environment that promotes the growth of anaerobic bacteria, often found in pilonidal cysts. The presence of bacteria and low oxygen levels hamper wound healing and exacerbate a forming pilonidal cyst.
Signs and symptoms
Pilonidal cysts are itchy and often very painful, and typically occur between
the ages of 15 and 35.[5] Although usually found near the coccyx, the condition
can also affect the navel, armpit, the cheek, or the genital region, though
these locations are much rarer.
Signs and symptoms may include:
- Intermittent pain/discomfort or swelling above the anus or near the
tailbone
- Opaque yellow (purulent) or bloody discharge from the tailbone area
- Unexpected moisture in the tailbone region
- Discomfort sitting on the tailbone, doing sit-ups or riding a
bicycle any activities that roll over the tailbone area
Some people with a pilonidal cyst will be asymptomatic.
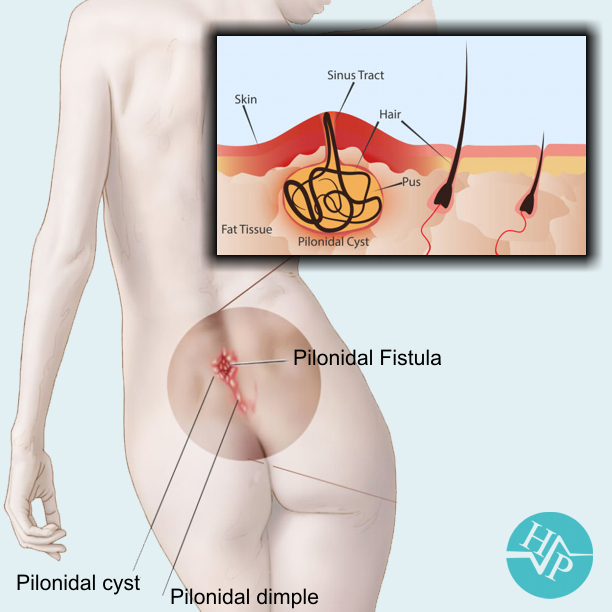
Pilonidal sinus
Pilonidal sinus (PNS): is a sinus tract, or small channel, that may originate
from the source of infection and open to the surface of the skin. Material from the cyst drains through the pilonidal sinus. A pilonidal cyst is usually painful, but with draining the patient might not feel pain.
Differential diagnosis
A pilonidal cyst can resemble a dermoid cyst, a kind of teratoma (germ cell tumor). In particular, a pilonidal cyst in the gluteal cleft can resemble a sacrococcygeal teratoma. Correct diagnosis is important because all teratomas require consultation with an oncologist and complete surgical excision, if possible without any spillage.
Treatment
Pilonidal cysts form a cavity below the surface of the skin that grows larger
over time and with recurrent cysts. This space is ideal for a lingering
infection, which is the reason that cysts often return.
Surgery is needed to remove all infectious material associated with the cyst,
and to close the cavity beneath the skin. There are two primary approaches to
closing the cavity:
Open healing The surgeon removes the cyst and leaves the cavity open to allow the tissue to
heal from the inside out. Healing usually takes a long time and is rarely
offered by surgeons at Progressive Surgical Care.
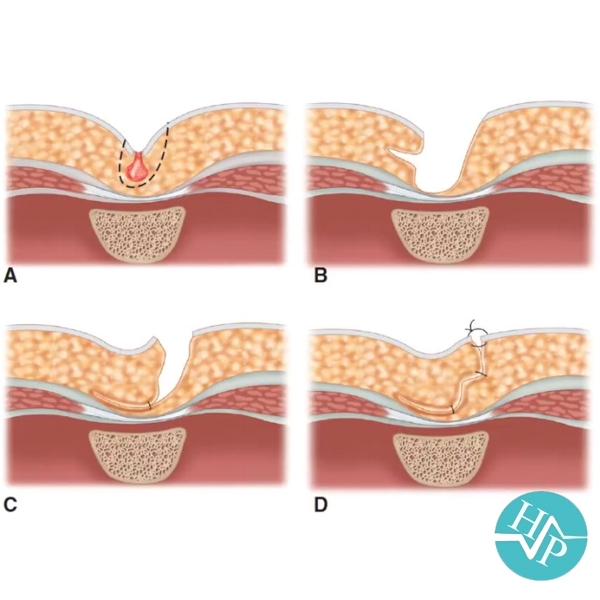
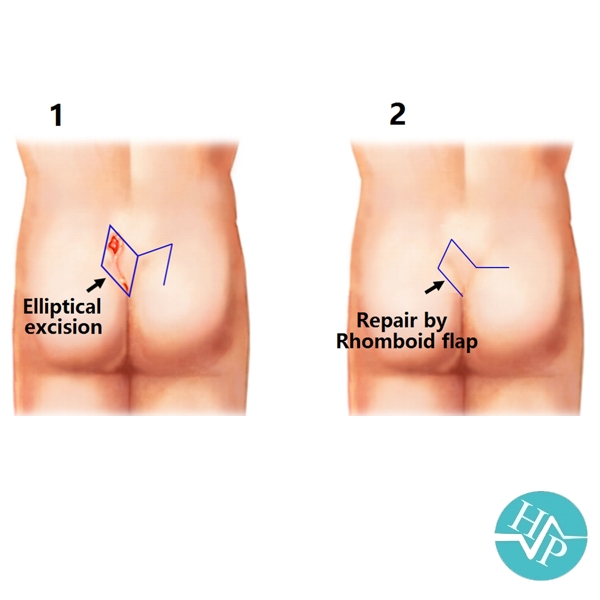
Primary closure The surgeon removes the cyst and then surgically closes the cavity using flaps
of muscle and skin. This seals the cavity and allows quicker healing.
Progressive Surgical Care utilizes the primary closure method. It's important to
follow your provider's post-operative instructions carefully, to ensure that you
heal effectively and prevent reinfection at the site. Their team is with you
every step of the way. Sutures are left in place for 10-14 days in this
sensitive area to assure complete closure.
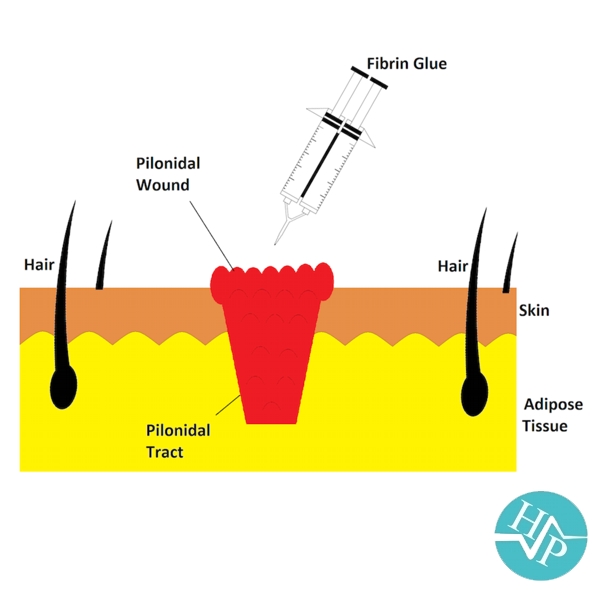
Fibrin glue injection is a method explored in recent years, with variable success. It involves injecting the fistula with a biodegradable glue which should, in theory, close the fistula from the inside out, and let it heal naturally.
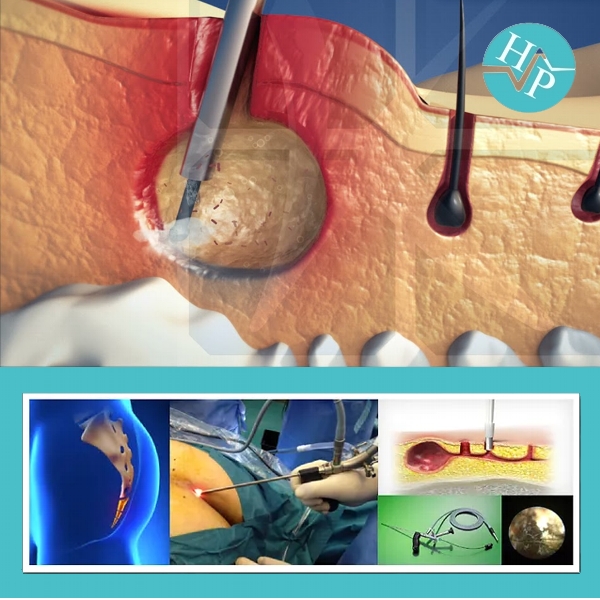
Endoscopic Pilonidal Sinus Treatment (EPSiT) is a
procedure less invasive surgery using a tiny camera to explore the sinus. The internal lining of sinus is safely burnt (cauterised) and cleaned with a brush. Some people will need more than once EPSiT for complete healing of sinus. This procedure is often performed as a day-case procedure under a brief general, spinal anaesthetic (awake anaesthesia with a needle injection into the back for patients with significant heart or lung diseases) or under local anaesthesia in selected patients.